Design Research
System Design
Agile Development
Vision Setting
UI/UX Design
Cardiovascular diseases exemplify the nation’s urban-rural health disparity. To address this, we created a scalable, AI-powered, health delivery system that dovetails the needs of the patients, the practice, and the technology.
My Role
In this 1.5-year, $1.6 million project, I partnered closely with the Primary Investigator Dr. Arruda-Olson to develop an intervention model appropriate for rural sites.
I led a co-design process where we leveraged methods such as staff workshops, patient interviews, and rapid prototyping to uncover the rural clinic’s capacities and limitations.
I coordinated the IT development team through an agile process for platform enhancements and redesigned the AI-powered platform to be role-oriented so that the information is actionable.
Additionally, my colleague and I co-created workflows with the rural clinic, visualized novel service processes, and operationalized the pilot study.
Process
Dr. Arruda-Olson’s informatics team spent five years developing an AI tool that could better detect patients who would benefit from cardiovascular prevention strategies. Cardiovascular diseases are 40% more prevalent in rural communities compared to urban areas. The needs of rural patients are different than their urban counterparts. Tailored interventions are needed.
We focused on co-designing with Mayo Clinic branch’s in Austin, MN. Austin’s embodies quintessential rural challenges such as an aging population and a shortage of providers. The AI platform could enable non-MD clinicians to deliver cardiovascular health prevention.
Participatory design played a key role in developing a context-relevant intervention to adapt the AI tool to rural clinical practices.

The process we used is visualized below:
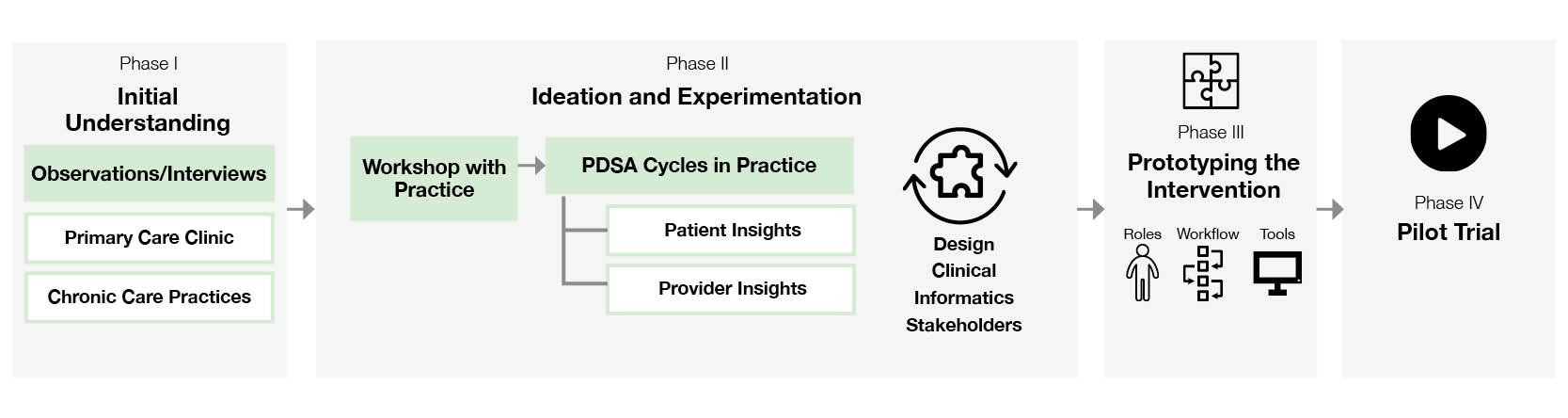
Initial Understanding
To understand the unique affordances and barriers of the rural clinic, we conducted:
- Workshops with staff to come up with experiments
- Interviews with patients to understand barriers
- Observations of chronic care visits across various departments
These initial engagement with staff helped us build rapport with the frontline clinicians and allowed us to identify motivated go-getters for the next phase.
Experimentation and Ideation
Our rapid prototypes within the clinic led to the key insight:
- “Day-to-day care is messy.” It’s difficult squeezing in cardiovascular conversations during in-clinic visits since time is already stretched thin. New, intentional touchpoints are needed.
Similarly, usability testing helped us understand what clinical information our care team members need to plan patient’s care, but :
- Care team members already have queues of patients to deal with. They don’t have time to manage a new workflow for the patients the AI tool is identifying.
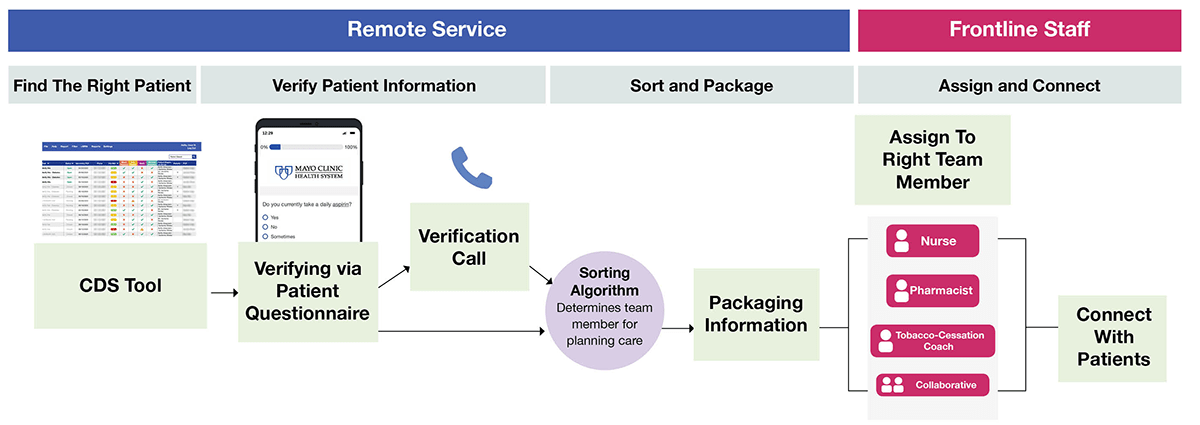
Prototyping the Intervention
Thanks to these insights, we reframed the intervention. A remote service would handle the clerical work of identifying the right patient, verifying the information, and sorting and sending the information to the right care team staff.
Piloting the Intervention
We spent 3 months piloting the intervention with a randomized controlled pragmatic pilot. During the pilot, we met weekly with the care team, iterating on their feedback. I facilitated Agile Development cycles with the IT team based on the practice’s input.

The pilot signaled promising results as 58% of eligible patients (88 out of 152) activated the intervention by completing a verification questionnaire. At completion of the 3-month pilot trial, 11% of patients implemented guideline recommendations, and 34% of eligible patients had preventive cardiovascular encounters that they may not otherwise have received.
Outcomes
By co-designing with a rural clinic and responding to its constraints, we developed a model that could scale to other sites. A Remote Hub could be set up in all regions of the Mayo Clinic health system to service all 47 branches.


Related Publications
Partogi M, Gaviria-Valencia S, Pick NJ, Bonacci RP, Mitchell JD, Chaudhry R, Swanson KM, Arruda-Olson AM. A Framework for Co-Designing Contextually Relevant Sociotechnical Interventions: Addressing Preventive Cardiovascular Health in Rural Settings. Poster presented at: AMIA 2021 Virtual Clinical Informatics Conference. 2021 May 18-20; USA.
Partogi M, Gaviria-Valencia S, Kessler M, Pick NJ, Chaudhry R, Arruda-Olson AM. Co-Designing an intervention for transformation of Cardiovascular Care Delivery in Rural Settings. Poster presented at: ACC Cardiovascular Summit Virtual. 2021 Feb 12-13. USA
Partogi M, Kaggal V, Pick NJ, Gaviria-Valencia S, Bonacci R, Michelle J, Chaudhry R, Hankey R, Franqueira A, Arruda-Olson AM. A Transformative Model for Cardiovascular Prevention in Rural Settings. Poster presented at: Mayo Clinic Artificial Intelligence Symposium. 2021 May 17-18. Rochester, Mn, USA.